Puma Biotechnology Presents Final Overall Survival Analysis from the Phase III ExteNET Trial at the 2020 SABCS
![]()
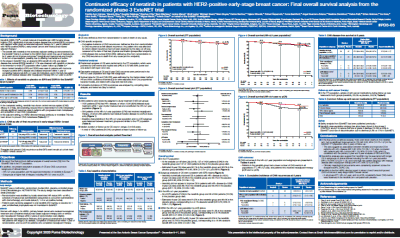
Results show continued efficacy of neratinib in patients with HER2-positive early stage breast cancer
LOS ANGELES, Calif., December 11, 2020 / B3C newswire / -- Puma Biotechnology, Inc. (NASDAQ: PBYI), a biopharmaceutical company, announced that efficacy results of neratinib in HER2-positive early stage breast cancer (eBC) from the Phase III ExteNET trial were presented at the 2020 Virtual San Antonio Breast Cancer Symposium (SABCS) that is currently taking place. The presentation entitled, “Continued efficacy of neratinib in patients with HER2-positive early-stage breast cancer: Final overall survival analysis from the randomized phase 3 ExteNET trial,” is being presented at a Spotlight Poster Discussion Session by Frankie Ann Holmes, M.D., FACP, Texas Oncology Houston – US Oncology Research, an investigator of the trial. A copy of this poster presentation is available on the Puma website.
ExteNET was a multicenter, randomized, double-blind, Phase III trial of 2,840 HER2-positive eBC patients who received neratinib after neoadjuvant and/or adjuvant therapy with chemotherapy and trastuzumab. Patients were stratified by hormone receptor status and randomly assigned to one year of treatment with either oral neratinib 240 mg/day or placebo. The primary endpoint of the trial was invasive disease-free survival (iDFS). Secondary endpoints include overall survival and cumulative incidence of CNS metastases. A descriptive analysis that evaluated CNS disease free survival, which was defined as time from randomization to any CNS recurrence or death from any cause, was performed.
Within the European Union, neratinib is approved in patients with hormone receptor positive (HR+) breast cancer who initiated treatment within one year of completing an adjuvant trastuzumab containing regimen.
The endpoints were analyzed for three groups of clinical interest: (i) the intent to treat (ITT) population; (ii) patients with HR+ breast cancer who initiated treatment within one year of completing an adjuvant trastuzumab containing regimen; and (iii) patients with HR+ breast cancer who initiated treatment within one year of completing an adjuvant trastuzumab containing regimen and who did not achieve a pathological complete response (no pCR) after neoadjuvant treatment and therefore were at a high risk of disease recurrence. Results from the Phase III ExteNET trial were published in the October 5, 2020 issue of Clinical Breast Cancer. The manuscript is accessible online at https://www.clinical-breast-cancer.com/article/S1526-8209(20)30258-5/fulltext.
In the ITT population, 127 of 1420 patients (8.9%) in the neratinib group and 137 of 1420 patients (9.6%) in the placebo group died, as of the analysis cut-off date (July 2019). The estimated 8-year overall survival (OS) rates were 90.1% in the neratinib group and 90.2% in the placebo group (stratified HR 0.95; 95% confidence interval [CI] 0.75-1.21; p=0.69). The cumulative incidence of CNS metastases at 5 years was 1.3% (95% CI 0.8-2.1) in the neratinib arm and 1.8% (95% CI 1.2-2.7%) in the placebo arm, while the estimated CNS disease free survival at 5 years was 97.5% in the neratinib group and 96.4% in the placebo group (stratified HR 0.73; 95% CI 0.45-1.17).
In the HR+ /< 1 yr patient population, 53 of 670 patients (7.9%) in the neratinib group and 68 of 664 patients (10.2%) in the placebo group died. The estimated 8-year OS rates were 91.5% in the neratinib group and 89.4% in the placebo group, corresponding to a 2.1% absolute benefit (HR 0.79; 95% CI 0.55‒1.13). The cumulative incidence of CNS metastases at 5 years was 0.7% (95% CI 0.2-1.7) in the neratinib arm and 2.1% (95% CI 1.1-3.5) in the placebo arm, while the estimated CNS disease free survival at 5 years was 98.4% in the neratinib group and 95.7% in the placebo group (stratified HR 0.41; 95% CI 0.18-0.85).
In the HR+/ <1 yr, no pCR subgroup of patients (n=295), 8-year OS rates were 91.3% in the neratinib group and 82.2% in the placebo group, corresponding to a 9.1% absolute benefit (HR 0.47; 95% CI 0.23–0.92). In the HR+/ <1 yr, with a pCR (n=38), 8-year OS rates were 93.3% in the neratinib group and 73.7% in the placebo group, corresponding to a 19.6% absolute benefit (HR 0.40; 95% CI 0.06–1.88). The cumulative incidence of CNS metastases at 5 years was 0.8% (95% CI 0.1-4.0) in the neratinib arm and 3.6% (95% CI 1.3-7.8%) in the placebo arm, while the estimated CNS disease free survival at 5 years was 98.4% in the neratinib group and 92.0% in the placebo group (stratified HR 0.24; 95% CI 0.04-0.92).
Dr. Frankie Ann Holmes said, “These descriptive analyses in HR+ patients who received neratinib within one year of completing trastuzumab and did not achieve a pCR post neoadjuvant therapy suggest that neratinib may be associated with improved OS in this high-risk group (HR 0.47, absolute benefit 9.1%). Importantly, neratinib is the first HER2-directed agent to show a trend towards improved CNS outcomes in early stage HER2-positive breast cancer, with consistently fewer CNS events observed in the neratinib arm compared with placebo in all groups evaluated.”
Alan H. Auerbach, Chief Executive Officer and President of Puma, added, “Descriptive analyses suggest that neratinib may be associated with longer overall survival in subgroups of clinical interest and in the high-risk patient subgroup with residual disease after neoadjuvant therapy who are at a high risk of disease recurrence. Although there have been many new treatment options for patients with early stage HER2-positive breast cancer, the risk of disease recurrence and more specifically CNS recurrence remains significant and more must be done. These newly published data demonstrate that neratinib provides a clinically meaningful reduction in the risk of recurrence and CNS recurrence and provides a very important option for these high risk patients.”
Click the image to get the Control Poster PDF.
About HER2-Positive Breast Cancer
Up to 20% of patients with breast cancer tumors over-express the HER2 protein (HER2-positive disease) and in the ExteNET study, 57% of patients were found to have tumors that were hormone-receptor positive. HER2-positive breast cancer is often more aggressive than other types of breast cancer, increasing the risk of disease progression and death. Although research has shown that trastuzumab can reduce the risk of early stage HER2-positive breast cancer recurring, up to 25% of patients treated with trastuzumab experience recurrence within 10 years, the majority of which are metastatic recurrences.
About Puma Biotechnology
Puma Biotechnology, Inc. is a biopharmaceutical company with a focus on the development and commercialization of innovative products to enhance cancer care. Puma in-licenses the global development and commercialization rights to PB272 (neratinib, oral), PB272 (neratinib, intravenous) and PB357. Neratinib, oral was approved by the U.S. Food and Drug Administration in 2017 for the extended adjuvant treatment of adult patients with early stage HER2-overexpressed/amplified breast cancer, following adjuvant trastuzumab-based therapy, and is marketed in the United States as NERLYNX® (neratinib) tablets. In February 2020, NERLYNX was also approved by the FDA in combination with capecitabine for the treatment of adult patients with advanced or metastatic HER2-positive breast cancer who have received two or more prior anti-HER2-based regimens in the metastatic setting. NERLYNX was granted marketing authorization by the European Commission in 2018 for the extended adjuvant treatment of adult patients with early stage hormone receptor-positive HER2-overexpressed/amplified breast cancer and who are less than one year from completion of prior adjuvant trastuzumab-based therapy. NERLYNX is a registered trademark of Puma Biotechnology, Inc.
IMPORTANT SAFETY INFORMATION
NERLYNX® (neratinib) tablets, for oral use
INDICATIONS AND USAGE: NERLYNX is a kinase inhibitor indicated:
- As a single agent, for the extended adjuvant treatment of adult patients with early-stage HER2-positive breast cancer, to follow adjuvant trastuzumab-based therapy.
- In combination with capecitabine, for the treatment of adult patients with advanced or metastatic HER2-positive breast cancer, who have received two or more prior anti-HER2 based regimens in the metastatic setting.
CONTRAINDICATIONS: None
WARNINGS AND PRECAUTIONS:
- Diarrhea: Aggressively manage diarrhea. If diarrhea occurs despite recommended prophylaxis, treat with additional antidiarrheals, fluids, and electrolytes as clinically indicated. Withhold NERLYNX in patients experiencing severe and/or persistent diarrhea. Permanently discontinue NERLYNX in patients experiencing Grade 4 diarrhea or Grade ≥ 2 diarrhea that occurs after maximal dose reduction.
- Hepatotoxicity: Monitor liver function tests monthly for the first 3 months of treatment, then every 3 months while on treatment and as clinically indicated. Withhold NERLYNX in patients experiencing Grade 3 liver abnormalities and permanently discontinue NERLYNX in patients experiencing Grade 4 liver abnormalities.
- Embryo-Fetal Toxicity: NERLYNX can cause fetal harm. Advise patients of potential risk to a fetus and to use effective contraception.
ADVERSE REACTIONS:
The most common adverse reactions (reported in ≥ 5% of patients) were as follows:
- NERLYNX as a single agent: Diarrhea, nausea, abdominal pain, fatigue, vomiting, rash, stomatitis, decreased appetite, muscle spasms, dyspepsia, AST or ALT increased, nail disorder, dry skin, abdominal distention, epistaxis, weight decreased, and urinary tract infection.
- NERLYNX in combination with capecitabine: Diarrhea, nausea, vomiting, decreased appetite, constipation, fatigue/asthenia, weight decreased, dizziness, back pain, arthralgia, urinary tract infection, upper respiratory tract infection, abdominal distention, renal impairment, and muscle spasms.
To report SUSPECTED ADVERSE REACTIONS, contact Puma Biotechnology, Inc. at 1-844-NERLYNX (1-844-637-5969) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS:
- Gastric acid reducing agents: Avoid concomitant use with proton pump inhibitors. When patients require gastric acid reducing agents, use an H2-receptor antagonist or antacid. Separate NERLYNX by at least 3 hours with antacids. Separate NERLYNX by at least 2 hours before or 10 hours after H2-receptor antagonists.
- Strong CYP3A4 inhibitors: Avoid concomitant use.
- Moderate CYP3A4 and P-glycoprotein (P-gp) dual inhibitors: Avoid concomitant use.
- Strong or moderate CYP3A4 inducers: Avoid concomitant use.
- P-glycoprotein (P-gp) substrates: Monitor for adverse reactions of narrow therapeutic agents that are P-gp substrates when used concomitantly with NERLYNX.
USE IN SPECIFIC POPULATIONS:
- Lactation: Advise women not to breastfeed.
Please see Full Prescribing Information for additional safety information.
To help ensure patients have access to NERLYNX, Puma has implemented the Puma Patient Lynx support program to assist patients and healthcare providers with reimbursement support and referrals to resources that can help with financial assistance. More information on the Puma Patient Lynx program can be found at www.NERLYNX.com or 1-855-816-5421.
Contacts
Puma Biotechnology, Inc.
Alan H. Auerbach or Mariann Ohanesian
+1 424 248 6500
info@pumabiotechnology.com
ir@pumabiotechnology.com
Russo Partners
David Schull or Maggie Beller
+1 212 845 4200
david.schull@russopartnersllc.com
maggie.beller@russopartnersllc.com
Keywords: Humans; Breast Neoplasms; neratinib; Clinical Trials, Phase III as Topic; Receptor, ErbB-2; Receptors, Estrogen; Trastuzumab; Survival Analysis; Disease-Free Survival; Neoadjuvant Therapy; Double-Blind Method
Published by B3C newswire
Editor Details
-
Company:
- B3C newswire
- Website:
